(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
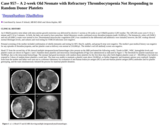
An O Rh(D)-positive term infant with intra-uterine growth restriction was delivered by elective C-section at 38 weeks to an O Rh(D)-positive G2P2 mother. The APGAR scores were 9 /10 at 1 minute and 9 /10 at 5 minutes. At birth, the baby was noted to have petechiae. Initial laboratory results confirmed severe thrombocytopenia (nadir 10,000/µL). The hematocrit, white cell (WBC) and red cell (RBC) counts were normal to low. Disseminated intravascular coagulation (DIC) was considered in the differential and antibiotics were initiated; however, the DIC workup showed normal fibrinogen levels, and cultures and viral testing for TORCH infections were negative.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A male newborn was delivered at gestational age 37 weeks and 1 day via spontaneous vaginal delivery. His teenage mother was G1P1 and received routine antenatal care. His mother's blood type was A- (for which Rhogam treatment was received) and her pregnancy was complicated by preeclampsia.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a woman is her late 30's with a history of recurrent scalp lesion. She presented to her PCP with a 3-day history of inflamed scalp lesion and an enlarged lymph node. Physical examination revealed erythematous skin breakdown at the crown to the right of the midline, but no drainage expressible. There was a large, tender right posterior auricular lymph node. She was treated with Bactrim DS for suspected scalp cellulitis. One week after her initial presentation, she developed a fever, jaundice, emesis and coca cola-colored urine. She presented to an outside hospital and was transferred to UPMC for further evaluation. On admission, she was hemodynamically stable. Physical examination revealed scleral icterus. Relevant laboratory results are shown below.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
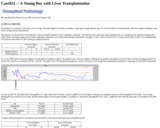
The patient is a young boy, less than 2 years of age, with end-stage liver disease secondary to glycogen storage disease, type IV, treated with liver transplantation. The liver segment allograft came from a living closely-related donor.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 60-70 year old male patient with a history of prostate cancer presented to the ED after being informed that they had abnormal findings on blood work drawn the previous day at their oncology appointment. Lab results showed a hemoglobin of 6.8. The patient denied any symptoms, including fatigue, dizziness, lightheadedness, chest pain or shortness of breath. The patient reported having consistently low hemoglobin values since receiving chemotherapy the previous year. A review of the patient's lab revealed a recent downward trend in the patient's hemoglobin values.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 20-30 year old female, gravida 2, para 1 who presented for follow up of an established pregnancy. The patient denied any symptoms, and has no history of prior blood transfusion or other significant medical history. She has one healthy child from the same marriage. The husband is healthy. Upon current pregnancy workups, including routine blood type and screen, the mother's blood group was found to be AB Rh positive with a positive antibody screen. Anti-Jka antibodies were identified with antihuman globulin (AHG) phase titers of 1:8. The mother was phenotyped and she is Jka negative. The father of the baby (FOB) was phenotyped and he is homozygous for Jka (Jka+Jkb-). The predicted phenotype of the baby is Jka+Jkb+.
No restrictions on your remixing, redistributing, or making derivative works. Give credit to the author, as required.
Your remixing, redistributing, or making derivatives works comes with some restrictions, including how it is shared.
Your redistributing comes with some restrictions. Do not remix or make derivative works.
Most restrictive license type. Prohibits most uses, sharing, and any changes.
Copyrighted materials, available under Fair Use and the TEACH Act for US-based educators, or other custom arrangements. Go to the resource provider to see their individual restrictions.