(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 51 year-old right-handed female presented with a two-month history of double vision and numbness around her left ear. Her walking became unsteady and she progressively developed left facial and tongue numbness, left-sided hearing loss and a left facial droop. In the two weeks prior to presentation she complained of headaches with associated nausea and vomiting.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 52 year old man with an unremarkable clinical history started to complain of daily somnolence, unusual irritability and some memory lapses. A few months later, he had fever and developed confusion with myoclonic jerks of the left limbs. Upon admission a diagnosis of encephalitis was made. MRI FLAIR images (Figure 1 A, B) showed cortical and sub-cortical abnormal signal intensity in parasagittal posterior frontal and anterior parietal regions, compatible with ischemic damage in watershed areas. On coronal T1-weighted image (insert in Figure 1A) cortex was hyperintense for petechial hemorrhage. Multivoxel Proton Magnetic Resonance Spectroscopy (1 H-MRS) demonstrated lactic acid in the lesions (Figure 1C, arrows). The CSF showed 10 white cells / ml with normal protein and glucose. He was treated with antibiotics, acyclovir, steroids and immunoglobulins and improved so that he was discharged to a rehabilitation facility. The patient could play chess and walk around with the help of a walking frame.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
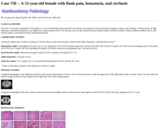
The case is received in consultation. The patient is a 52-year-old female who presented to her primary care physician with presyncopal symptoms, nausea, and vomiting. A further history of right flank pain, intermittent hematuria, and weight loss of approximately 20 lb. over the past year was also elicited. Her past medical history includes alcoholic cirrhosis, diabetes mellitus type II, and thyroid surgery with thyroid hormone replacement therapy.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 52 year old female came with intermittent left facial paresthesia/ hyperesthesia and swelling since 3 weeks.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 52-year-old male who presented to gastroenterology with a 3 week history of abdominal pain. He described the abdominal pain as sharp, mid upper abdominal pain that occurred immediately after meals and was not relieved by over-the-counter antacids or pain medications. He had some heartburn, but denied other gastrointestinal symptoms. A colonoscopy was performed and showed a large intraluminal mass in the proximal ascending colon. A biopsy was performed but was not representative of the mass. A right hemicolectomy was performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was a 52 year old male with a history of Cushing's disease, initially diagnosed at the age of 18. At that time, his symptoms included increased weight, purple abdominal striae, diabetes mellitus, and polydipsia. He underwent a resection of a pituitary microadenoma at another hospital. However, due to persistently high cortisol levels following the surgery, he later underwent a bilateral adrenalectomy. Following the operation, he began hydrocortisone therapy, lost weight, and was able to maintain glucose control without diabetes medications. At the age of 32 his diabetes recurred, but he was able to maintain good glucose control up until age 51 at which time his HbA1C was greater than 7. He also had visual problems with significant reduction in right peripheral vision and moderate impairment in left. Testing revealed a greatly elevated serum ACTH at 5,082 pg/mL (normal is 9 - 46 pg/mL), but serum cortisol within normal limits 4 ug/dL. There was no pigmentation of the skin. MRI scans found a large, contrast-enhancing mass in the pituitary fossa with extrasellar extension into the right cavernous sinus and displacement of the parasellar carotid posteriorly (Figs 1 and 2). The patient underwent endoscopic endonasal approach for debulking of the mass.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 52-year-old man was admitted with dyspnea and found to have pneumonia. He was treated and discharged but continued to be dyspneic, with new symptoms of fever, night sweats, and weight loss, leading to readmission one month later.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 53-year-old woman presented with a growing mass in the left lumbar region. The patient had become casually aware of it ten years ago. Since then she performed radiological and clinical follow-up; she refused surgical resection. In 2009 a cytological examination had displayed mesenchymal cells without nuclear atypia. In the last year the tumor had been growing and had become symptomatic with pain during physical activity. Clinical examination revealed an unmovable swelling on the left lumbar region with intact skin. MRI showed a 9x4x5 cm T1 hypointense and T2 hyperintense mass, with a strong and heterogeneous enhancement after contrast infusion and a hypointense central core. It extended from the body of the second to the fifth lumbar vertebra. CT scan of the chest also revealed four pulmonary nodules enhancing with contrast, two of which were hypermetabolic during the whole body PET-CT scan (max SUV 2.7 and 2.4). The patient underwent surgical resection of the lumbar lesion which was easily removed with sharp dissection from the surrounding muscle fibers.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
DL is a 53-year-old male with past medical history significant only for hepatitis C. He was discovered one afternoon convulsing and unresponsive in a cemetery. He was initially taken to UPMC Northwest, where he was intubated for airway protection and loaded with phenobarbital 1 gram IV to treat the diffuse muscle spasms. His vital signs at this time included a temperature elevated to 39.0oC, a blood pressure of 143/74 mm Hg, a heart rate of 120 beats per minute, respiratory rate of 17 breaths per minute, and an oxygen saturation of 100%. An arterial blood gas demonstrated profound combined metabolic and respiratory acidosis with pH 6.55 (reference range 7.35-7.45), pCO2 92 mm Hg (reference range 35-48 mm Hg), pO2 368 mm Hg (reference range 83-108 mm Hg), HCO3 10 mEq/L (reference range 22-26 mEq/L). He was transferred to UPMC Presbyterian for further management.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 53-year old male who presented to the emergency room with a five day history of worsening rash, pain and swelling in his right hand that had progressed to include facial and left hand involvement.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 53 year old male who presented with intermittent fevers, night sweats, and a chronic cough. The patient underwent a PET scan, which showed an enlarged supraclavicular lymph node, a lesion in the left lobe of his liver and bulky retroperitoneal lymphadenopathy. His peripheral blood showed a normocytic normochromic anemia with leukocytosis. The patient underwent excision of the supraclavicular lymph node.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 53-year-old male was found to have leukocytosis and a neutrophilic left shift on routine blood work (Image 1).
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 53-year-old obese man was transferred to the hospital with new onset seizures and a left frontal intracranial tumor diagnosed by a CT scan. The preceding medical history was significant for chronic obstructive pulmonary disease, asbestos exposure, 30-pack-years of tobacco use and chronic alcoholism.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was a 53 year-old man who presented with confusion and amnesia and subsequently suffered rapid progressive cognitive decline over the next few weeks associated with myoclonic jerks. His condition did not improve and he expired just over 3 years after presentation. The patient had a past medical history of adult onset generalized epilepsy beginning the third decade of life. Initially the cognitive decline, myoclonic jerks and epilepsy were not thought to be linked and a clinical diagnosis of Creutzfeldt-Jakob disease was made based on the age of onset symptoms and the aggressive nature of the disease.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 53 year old man presented with a cyst on his left cheek. The lesion was excised and submitted with a postoperative diagnosis or "epidermal inclusion cyst."
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 53-year-old white male with a history of alcohol abuse and pancreatitis presented to the emergency department with a 6-month history of nausea, vomiting and weight loss. One month prior, he had been diagnosed with cirrhosis of the liver, and subsequently hospitalized twice with removal of two and then five liters of ascites fluid. He developed significant abdominal pain associated with nausea and vomiting. He also had difficulty tolerating oral intake and constipation. He was not eating but sustaining himself on fluids. On physical examination, the patient was not jaundiced, but his abdomen was distended with a positive fluid wave. A firm mass was noted in the left mid epigastrium judged consistent with splenomegaly. His total bilirubin was 0.5 (direct 0.1), alkaline phosphatase 102, ALT 27, AST 17, albumin 3.4, total protein 6.3, prothrombin time 9.4, INR 1, partial thromboplastin time 33.8, amylase 257 and lipase 1130. He was admitted with a diagnosis of acute pancreatitis. He was made n.p.o. and given IV fluids.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 53-year-old woman presented with a 1-month history of severe headache and intractable vomiting. Physical examination revealed left facial palsy and generalized weakness of the extremities (grade IV/V all extremities) without other localizing signs. She had no known underlying disease and there was no significant family history. MRI of the brain disclosed multiple ill-defined high signal lesions in T2W at left lower pons, left thalamus, subcortical regions of temporal, parietal, and frontal lobes bilaterally, and periventricular white matter. Nodular enhancement was noted in the left frontal lobe lesion (Figure 1), left thalamus (not shown) and left pons (Figure 2). Irregular leptomeningeal enhancement was also noted diffusely. The largest mass present at the left frontal lobe was 2 cm in largest dimension and showed marked peritumoral vasogenic edema (Figure 1). High resolution chest CT revealed an ill-defined mass at the posterior basal segment of the right lower lobe, 3.2 cm in greatest dimension (not shown). There were also multiple small nodules involving both lungs, ranging from 0.4 to 0.5 cm. Stereotactic biopsy of the left frontal lobe lesion was performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 54-year old male presented with left vision loss, headache and left-sided facial pain. On physical examination medial and inferior displacement of the left eye was noted. He had a remote history of intracranial surgeries 17 and 5 years prior to this admission which included a left frontotemporal craniectomy, partial resection of the left anterior temporal lobe and sinonasal surgeries. Magnetic resonance post-contrast images showed enhancing lesions on the left side adjacent to the optic nerve, in the anterior temporal lobe, fronto-ethmoid sinus (Figure 1A), parasellar region, skull base, right dura, nasal cavities, and nasopharynx. A body positron emission tomography scan demonstrated evidence of tumor in the left deep cervical lymph nodes. Eight months later, intradural masses were noted in the cauda equina, thoracic paravertebral region and in the lumbar vertebral bodies. The nasopharyngeal mass was biopsied.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A fifty-four year old female with past medical history of pulmonary hypertension, fibromyalgia, chronic obstructive pulmonary disease, coronary artery disease and hypertension presented to the emergency department with complaints of increased dyspnea, lower extremity edema, weight gain, orthopnea, fevers, chills, night sweats over the past few months. She denied any cough or sputum production. The patient was on trepostinil (remodulin) infusion since 3 years. She had a history of line infection two years ago which was successfully treated with antibiotics. Patient had a right subclavian port placed about ten months ago. Her other medications included estrogen, escitalopram, warfarin and gabapentin. The patient did have a remote history of smoking although she had quit smoking eight years prior. She denied any drug allergies, alcohol or intravenous drug abuse.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
This is a 54-year-old white male with a history of polymyositis, type 1 diabetes mellitus, and hypothyroidism who has been on immunosuppression with methotrexate and prednisone. He presented with an episode of vomiting, headache, memory loss, cognitive decline, and right lower extremity weakness and numbness that lasted for about four hours, three days prior to admission. The symptoms were resolved spontaneously after sleep.
No restrictions on your remixing, redistributing, or making derivative works. Give credit to the author, as required.
Your remixing, redistributing, or making derivatives works comes with some restrictions, including how it is shared.
Your redistributing comes with some restrictions. Do not remix or make derivative works.
Most restrictive license type. Prohibits most uses, sharing, and any changes.
Copyrighted materials, available under Fair Use and the TEACH Act for US-based educators, or other custom arrangements. Go to the resource provider to see their individual restrictions.