(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 12-year-old male presented with a 14-month history of progressive weakness of his right arm and leg as well as a deviated mouth. Physical examination revealed a mild right-sided central facial palsy and mild right hemiplegia. MRI axial T1 images showed a mixed and ill-defined signal in left thalamus and cerebral peduncle with mild speckled enhancement (Figure 1a). The anterior horn of the left lateral ventricle and left lateral fissure were enlarged as compared with contralateral side (Figures 1a, 1b). The left cerebral peduncle was significantly smaller than that on the right (Figures 1c, 1d). A stereotactic needle biopsy was performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
12 year-old boy without significant past medical history presented with substernal chest pain. He was diagnosed to have left lower lobe pneumonia and was receiving oral antibiotics for 2 days prior to this referral. His chest pain subsided after albuterol nebulizer treatment in a local hospital, but he was found to have elevations of cardiac troponin I (cTnI) and creatine kinase (CK)-MB with ST changes on electrocardiogram (ECG), and was referred for further evaluation.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
Clinical history-1 This 12-year-old boy presented with a one-month history of intracranial raised pressure syndrome, characterized by headache and vomiting, followed by nuchal pain and torticollis. Physical and neurological examinations were normal except for papilledema. No hereditary syndromes were disclosed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was the product of a normal pregnancy and birth and followed normal developmental milestones apart from some difficulty with fine motor skills. She walked and talked at 1 year of age. At the age of 7 years, she had an episode of generalized convulsive status epilepticus, and was told that she had suffered from a viral encephalitis. She developed recurrent seizures at the age of 8 years. A decline in school performance was noted around this time. At 10 years of age, the seizures became more frequent, and she developed a global developmental regression, with loss of language and cognition. She also developed a movement disorder with chorea and myoclonus.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
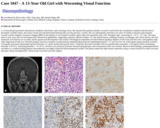
A 13-year-old girl presented with polyuria, headache, drowsiness, and worsening vision. She reported that polyuria initially occurred 5 years before the consultation, headache and drowsiness developed 3 months earlier, and vision in both eyes had deteriorated dramatically over the previous 1 month. She was subsequently referred to our clinic for further evaluation and treatment. Coronal contrast magnetic resonance imaging (MRI) of the pituitary in our hospital revealed a giant sellar and suprasellar mass with "hourglass sign", measuring 25 × 42.2 × 23.7 mm. The mass had no cystic areas and was heterogeneously enhanced by gadolinium, suggesting a pituitary adenoma (Figure 1a). She denied nausea, vomiting, lactation, acromegaly, and central obesity. Her first menstrual cycle had not yet occurred, and her growth and development were normal. Neurological examination revealed bilateral pupillary dilation of OD 8 mm and OS 6 mm, with pupillary light reflex depressed in both eyes. Baseline pituitary function evaluation revealed primary hypothyroidism (thyroid-stimulating hormone: 7.17 μIU/ml, free-T4: 0.454 ng/dl), hypocortisolism (cortisol < 0.50 μg/dl), decreased somatotropin (growth hormone: 0.1 ng/ml, insulin-like growth factor: 133ng/ml), decreased estradiol with low gonadotropins (estradiol: 13.32 pg/ml, follicle-stimulating hormone: 0.20 IU/L, luteinizing hormone: < 0.2 IU/L). However, her prolactin, β-human chorionic gonadotropin, and α-fetoprotein levels were normal. Based on these findings, panhypopituitarism secondary to a nonfunctioning pituitary macroadenoma was highly suspected and presumptively treated. The patient underwent right frontal craniotomy using a coronal incision for tumor resection and optic chiasm decompression. Visual acuity recovered soon after surgery.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was a normally developing boy who noted hand tremors at 7.5 years of age, approximately 3 weeks after his last mumps, measles and rubella vaccine. One month later, he exhibited difficulty walking, leg pain and weakness. His gait became stiff legged with the right leg rotated outwards. He was found to have significant action and sustention tremor, bilateral lower leg weakness (tibialis anterior), decreased deep tendon reflexes and pes planus. He also exhibited impaired speech articulation.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
An 13-year-old female with a past medical history of attention deficit hyperactivity disorder and auditory processing impairment, who presented with refractory seizures. She had mild cognitive delay, necessitating enrollment in special education classes. She began having absence seizures around the age of 8 years. Her seizure disorder subsequently progressed to include generalized tonic-clonic seizures, resulting in an associated decrease in the level of verbal communication. She had no other known medical problems and an unremarkable family history. She presented for mapping of her seizure activity and subsequent lobectomy. Her long-term electroencephalogram (EEG) monitoring showed multiple patient events associated with rocking movements, but no time length correlation with associated behavioral events. There were multiple bursts of 8 to 10 Hz activity followed by 2 to 3 Hz activity and some secondary generalization.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was a 13-year-old girl with a long standing history of frequent headaches and a recent syncopal event. The syncope lasted for about 10 seconds with no seizure like activities. There were no complains of fevers/chills, nausea/vomiting/diarrhea, chest pain, short of breath or any other neurological symptoms. Family history was not significant.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 13 year old girl, product of an uncomplicated pregnancy, born at full-term (3620g, 53.3cm '50 percentile). Apgar scores are unknown. Examination at birth was otherwise unremarkable. She has always had short stature. She did not progress on the growth chart. A bone age done in August 2005 (chronological age 10 yo) by her primary care physician yielded 6 years and 10 months.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A right-handed 14 year-old boy was admitted for a first unprovoked generalized tonic clonic seizure, which was preceded by ongoing headache and nausea for a few days. His parents also noted a sharp decline in his academic performance in recent months. Physical examination was unremarkable except for the presence of right homonymous superior quadrantanopia. Psychological assessment revealed impairment in his verbal memory and learning. Blood results and EEG were unremarkable. Imaging of the brain by CT showed a left temporal mass with calcifications and hemorrhage (Figure 1), and MRI revealed a large avidly contrast-enhancing left temporal mass measuring 4 x 5 x 4cm with evidence of recent hemorrhage (Figures 2 and 3). There were foci of edema and mass effects causing compression of the left temporal horn with adjacent sulcal effacement (Figure 4). He underwent gross total tumor resection under ultrasound guidance via a left temporal craniotomy.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient, a 14-year-old with hypothyroidism since birth for which he was taking Synthroid (Levothyroxine), developed a nodule in the right lobe of the thyroid. The clinical working diagnosis was autoimmune thyroiditis. The family history was non-contributory. An ultrasound scan showed a hypoechoic nodule, and the thyroid function tests were all within normal limits. A fine needle aspiration was non-diagnostic; hence a right thyroid lobectomy was performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 14-year-old girl with a recent history of sciatica and ataxic gait was admitted to the Pediatric Neurosurgery service. Brain and spine MRIs revealed a mildly heterogeneously contrast-enhancing mass with a cystic component in the 4th ventricle with caudal extension through the foramen of Magendie with compression of the medulla (Figure 1A). Another cystic mass with a large enhancing nodule was detected in the left cerebellar hemisphere (Figure 1B). The spinal MRI revealed an extensive septated syrinx as well as an intramedullary contrast-enhancing nodule at T4 (Figure 1D). Diffuse leptomeningeal enhancement with scattered nodules was visible in the suprasellar cistern, internal auditory canals, interpeduncular fossa, the ventral brainstem as well as the spinal cord. Moreover two solid, contrast-enhancing lesions were detected in the right temporal lobe (Figure 1C); and in the sacral spinal cord, a "drop" metastasis was detected within the thecal sac (Figure 1E). A specific radiological diagnosis was not achieved. Multiple biopsies of the cerebellar lesion and of the tissue in the thecal sac were performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
Our patient is a 15 year-old boy, with a previous diagnosis of neurofibromatosis type 2, who had undergone surgical resections of olfactory groove tumors, at five and 13 years of age. Both resections had histopathologically-confirmed meningothelial meningioma (WHO grade I).The patient also had other intracranial lesions bilaterally in the cerebellopontine angle, and in the left Mackel cave, involving the vestibular and trigeminal nerves. All of these lesions showed enhancement with MRI. The patient suffered left hearing loss and left hemiparesis since the first surgery 10 years ago. Three months before admission, the patient developed seizures and antiepileptic drugs were introduced. MRI showed relapse in the olfactory groove lesion (Fig. 1a). At this time, a third microsurgical approach of the olfactory groove lesion was performed, achieving satisfactory resection (Fig. 1b). The patient's condition did not worsen postoperatively.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 15 year old boy presented to our center with progressive headache, vomiting, gait instability and reduced visual acuity of one month's duration. The patient related a head injury as a result of a fall while playing hockey as coinciding with the onset of his symptoms but no other significant history. Physical examination revealed severe bilateral papilledema.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 15 year-old female presented to the Emergency Room with urinary retention and inability to walk. She had developed progressive low back pain and bilateral leg pain about 2 months prior to presentation. Physical examination demonstrated bilateral positive Babinski reflex, bilateral positive Hoffmann's reflex, positive Romberg reflex and positive bulbocavernous reflex. Sagittal T1 weighted MRI scan post Gadolinium (Gd) using fat saturation technique showed an intensely enhancing intraspinal, extradural, 6.5 X 0.8 X 2.3 cm (cranial-caudal, anterior-posterior, transverse) mass, with anterior displacement and compression of the spinal cord (Figure 1A). The mass extended from T3 to T7. Axial T1 weighted MRI scan post Gd at T5 showed bilateral transverse process and spinous process involvement (Figure 1B). Axial T1 weighted MRI scan after Gd showed enhancing tumor in the spinal canal and neural foramina from T4 to T7 (Figure 1C, scan was taken at T5). A decompression surgery was performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 15-year-old girl presented to our institution with headache, vomiting, and nausea of 3-week duration. Physical examination showed no focal neurologic deficits. The patient's past medical, surgical, and family histories were all noncontributory.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 15-year-old adolescent male with a history of developmental delay who presented at 8 to 10 years of age with loss of peripheral vision and night blindness, at which time he was diagnosed with retinitis pigmentosa. He then developed progressive loss of central vision and macular edema. He was evaluated by an ophthalmologist, subspecialzing in genetics. A diagnostic laboratory test was requested because of the atypical presentation of retinitis pigmentosa.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 16 month old female was admitted to the Pediatric Intensive Care Unit with fever, hypoxia, altered mental status, and seizures. Magnetic resonance imaging (MRI) of the brain (Figure 1) showed a single well circumscribed intraventricular mass which was isointense to cortex on T1-and T2-weighted images, and demonstrated mildly restricted diffusion consistent with dense cell packing. The mass measured 4x4x4 cm in the craniocaudal, AP and transverse dimensions. FLAIR imaging revealed mass effect secondary to the tumor causing trapping of the left temporal horn. There was additional, but mild right lateral ventricular dilatation and an 11 mm midline shift as measured at the level of the anterior portion of the third ventricle. Edema was seen along the corpus callosum, surrounding the mass extending into the left occipital lobe, temporal lobe, and parietal lobe. These signal characteristics were most suggestive of an intraventricular meningioma or a supratentorial primitive neuroectodermal tumor.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 16-year-old right-handed male presented to an emergency room after suffering mild head trauma from a fall onto his head while intoxicated with alcohol. Physical examination revealed a healthy, inebriated male with no focal neurological deficit. The mother reported that her son had experienced excessive fatigue over the last three months. The patient's past medical, surgical and family history were all noncontributory.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
Patient is a 17 weeks gestational age fetus with significant shortening of long bones.
No restrictions on your remixing, redistributing, or making derivative works. Give credit to the author, as required.
Your remixing, redistributing, or making derivatives works comes with some restrictions, including how it is shared.
Your redistributing comes with some restrictions. Do not remix or make derivative works.
Most restrictive license type. Prohibits most uses, sharing, and any changes.
Copyrighted materials, available under Fair Use and the TEACH Act for US-based educators, or other custom arrangements. Go to the resource provider to see their individual restrictions.