(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 68-year-old woman was admitted to the Department of Neurosurgery because of sudden development of fluent aphasia after a history of about 20 days of right inferior-temporal quadrantanopia with left eye sight deterioration. MRI found a 3 cm hyperintense, contrast-enhancing mass in the left posterior-lateral orbital wall protruding through the optic foramen and displacing the temporal lobe (Fig. 1a). A meningioma was suspected and patient underwent left pterional craniotomy combined with a lateral orbitotomy in order to remove both the intraorbital and the intradural components of the tumor. The mass showed neither a clear dural implant, nor a well-defined dissection plan from the brain parenchyma, raising the suspicion of a lymphoproliferative disorder. Since the intraoperative pathological findings from frozen sections were suggestive for an inflammatory disease, only a partial resection was achieved to avoid damage to the optic nerve. The patient recovered well and was discharged with a left eye sight improvement.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
68 year old female presented with acute appendicitis. She had chief complaints of fever, nausea, vomiting and abdominal pain which had got worse 2 days before admission. Her past medical history was positive for hypertension. She underwent an emergency appendicectomy as she had developed signs of peritonitis.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
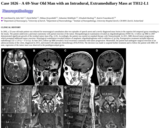
A 68-year-old diabetic male patient was initially admitted due to left-sided hearing loss, balance impairments and left-sided facial palsy in 2001. At that time he had been complaining of left-sided tinnitus for years. An MRI showed a mass in the cerebellopontine angle on the left side, causing mild compression of the brainstem. He underwent neurosurgery in 2002. The operation revealed that the 7th and 8th cranial nerves were profusely infiltrated by the tumor. The mass was excised by retrosigmoidal craniotomy and both nerves were preserved. Postoperatively, facial nerve palsy was still apparent. Gait and eyelid closure improved thereafter, whereas anacusis showed no improvement. He then underwent annual follow-up examinations. In 2006 T1-weighted horizontal MRI with gadolinium contrast enhancement demonstrated tumor recurrence (Fig. 1). Moderate increase in growth was seen in 2007 (Fig. 2), but surgical intervention was not indicated at that time. In 2010 the patient suffered from increasing dizziness and balance impairment. MRI examination revealed tumor growth with medial expansion and brainstem compression (Fig. 3) and second operation was performed. The tumor was again localized within the caudal cerebellopontine angle compressing the caudal brainstem and cranial nerves as well as the left crus cerebelli. On craniotomy the tumor was almost completely extirpated with a small residue remaining attached to the caudal cranial nerves. After operation, slight paresis of the 6th cranial nerve and hoarseness occurred.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
Our patient is a 68-year-old man who was transferred to this hospital with upper gastrointestinal (GI) bleeding. His medical history was significant for follicular lymphoma involving a left supraclavicular lymph node diagnosed 7 months prior to another lymphoma involving the right chest wall. Lymphoma of the chest wall preceded the upper GI bleeding by 2 months. Treatment for the lymphomas included 6 cycles of CHOP and local radiation to the chest.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 68 year old Caucasian male with COPD and left heart dysfunction who presented with a longstanding history of urinary urgency, frequency, and nocturia. He was diagnosed with high grade bladder outlet obstruction, but had a negative cystoscopic examination. Laboratory evaluation was remarkable for a prostate-specific antigen (PSA) of greater than 40 ng/mL, an increase from 32 ng/mL a year previously.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
This patient is a 68-year old female with a right parotid mass. No additional history was available. Parotidectomy was performed. Specimen consisted of a 4.5 x 4 x 1.3 cm parotid containing a 0.6 cm poorly demarcated firm white-tan nodule.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
In 2002, a 55-year old male patient was referred for neurosurgical consultation after two episodes of speech arrest and a newly diagnosed mass lesion in the superior left temporal gyrus extending to the insula. The patient underwent a pterional craniotomy with partial resection of the tumor. Histopathological examination revealed an oligodendroglioma (WHO II). A follow-up MRI in 2007 demonstrated significant growth of the residual tumor mass (Fig. A-D). Accordingly, the patient was started on standard therapy with Temozolomide. In 2011, MRI showed tumor progression, which prompted additional tumor resection. Histological examination revealed features of anaplastic oligodendroglioma with co-deletion of 1p/19q. Postoperative treatment included adjuvant radiotherapy (32 x 1.8 Gy = 57.6 Gy). In June 2015, follow-up MRI revealed a local recurrence consistent with tumor progression. Meanwhile, the patient had undergone surgical resection of an adenocarcinoma of the colon, diagnosed in 2015, and treated with adjuvant chemotherapy (FOLFOX4). The decision was made to suspend further treatment and to follow the patient with MRI. Of note, regression of the tumor mass was observed in the parahippocampal gyrus.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 69 year old African American female on hemodialysis for chronic renal failure was found to have a 2.6cm enhancing renal mass in the posterior right renal mid pole on abdominal CT scan. The patient underwent a laparoscopic nephrectomy. Her past medical history is significant for diabetes, hypertension, coronary artery disease status post coronary artery bypass graft and hyperlipidemia.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
This 69-year-old man with a past medical history notable for hypertension, chronic renal insufficiency, spinal stenosis and chronic back pain presented with a 40-pound weight loss due to decreased appetite and with intermittent left chest pain radiating to his left back of approximately one month's duration. A week prior to his admission, he became increasingly confused and weak and fell multiple times at home.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 69-year-old man presented with a left neck mass. The patient underwent total thyroidectomy, central compartment neck dissection, sternocleidomastoid muscle flap reconstruction, and primary closure of the esophageal wall. The total thyroidectomy specimen was irregular in shape, the right lobe measured 4.5 x 2.0 x 1.5 cm and the left lobe measures 9.0 x 5.5 x 4.5 cm. The exterior surface of the gland was tan-pink and rubbery. The cut surface of the left lobe revealed a 7.5 x 4.5 cm tan-grey lesion. The lesion approached to within less than 1mm of the capsular surface. Scant normal appearing thyroid parenchyma was present at the superior aspect of the left lobe. The right lobe parenchyma was red and beefy.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 69-year-old patient with a four-year history of CIDP was admitted for evaluation of further treatment options at a tertiary University hospital. Diagnostic criteria for CIDP established by the AAN were fulfilled [1]. Six months prior to this admission, the patient had suffered from a granulocytic meningitis while he was treated with azathioprine and prednisolone . At that time, evaluation of his cerebrospinal fluid (CSF) revealed a pleocytosis of 1240 white blood cells (WBC)/µl. Immunosuppressive therapy was immediately suspended. The causative pathogen could not be identified, but the patient partially recovered after empiric antibiotic treatment with ceftriaxon and ampicillin. Residual neurological deficits included persisting mild cognitive impairment. At that time, a cranial computer tomography (CT) and a magnetic resonance imaging (MRI) scan of the brain were normal.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 69 year old female with a history of bilateral breast cancer. In late 1995, she underwent a segmental mastectomy of the left breast that demonstrated invasive ductal carcinoma. Immunohistochemical staining was interpreted as borderline expression of estrogen receptor and negative expression of progesterone receptor. A few months later, in early 1996, she underwent a right total mastectomy with axillary dissection for invasive ductal carcinoma with a lobular component and signet ring features metastatic to thirteen out of thirteen axillary lymph nodes. The tumor in the left axillary lymph nodes was morphologically similar to the tumor of the left breast. Given that the mass of the right breast shared only part of the features of the left breast carcinoma, a second primary could not be ruled out. She was also treated with Tamoxifen, chemotherapy and radiation therapy to the right chest wall and left breast.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 69-year-old woman presented with a 2-month history of progressive bilateral leg weakness and gait difficulty. On examination, the patient had diffuse lower extremity weakness and hypesthesia of the left leg. Magnetic resonance imaging revealed a 2.9-cm, extradural, soft tissue mass at the T5-6 level, with spinal cord compression; the mass was hypointense on a T1-weighted image (Figure 1) and hyperintense on a T2-weighted image (Figure 2). The tumor was a relatively well-demarcated epidural mass with focal invasions into both facet joints. Intraoperative examination showed a neoplasm with clear and granular cell morphologies displaying solid, papillocystic, and follicular patterns. Postoperative 18F-fluoro-2-deoxy-D-glucose positron emission tomography-computed tomography (CT) and neck CT failed to identify a primary tumor or any other lesions.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 6-year-old female was admitted for fever, rectal bleeding, and a worsening of her long-standing abdominal pain. Her history consists of a multi-visceral transplant (partial stomach, small bowel, large bowel, pancreas, and liver) at age 2 secondary to microvillous inclusion disease. The patient has had multiple issues with her transplant including TPN-induced liver damage, multiple episodes of mild and moderate acute cellular rejection and adenovirus enteritis, low-grade EBV enteritis and colitis, Candidal esophagitis, and gastritis.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 6-year old girl with past medical history significant for biliary cirrhosis secondary to extra hepatic biliary obstruction (biliary atresia) who, at one year of age, underwent an cadaveric, orthotopic liver transplant (OLTx). The recipient's EBV status prior to transplantation was not available in the clinical records. Post-transplant serology was positive for EBV. Around 40 months post-transplantation, she had an episode of early EBV-associated PTLD of the adenoids which clinically responded to decreased immunosuppression. At 63 months post-transplantation, she presented with an enlarging left neck nodal mass that was surgically excised.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 6-year-old Japanese girl presented with psychomotor seizures including oral automatism with cloudy consciousness, lasting for 2 months. On admission, no neurological deficit was evident except for seizures, and no abnormal manifestations of the skin were observed. Magnetic resonance (MR) images indicated a tumor with peritumoral edema in the left middle cranial fossa, displaying heterogeneous enhancement with intravenous administration of gadolinium. The medial part of the tumor consisted of an irregular-shaped region, which was hyper-intense on T1-weighted images and hypo-intense on T2-weighted images (Fig. 1), indicating the presence of certain substances that shorten both T1 and T2 relaxation times, such as melanin, calcium and intracellular methemoglobin (4). This region was highlighted as a high-density area on computed tomography (Fig. 2). The patient underwent tumor resection through a left occipital craniotomy. The tumor was an extra-axial mass with focal blackish coloration in its medial portion, and intraoperative frozen sectioning showed a proliferation of pigmented cells among thick collagen fibers.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A previously healthy 6 year-old girl presented to the emergency department with gradually worsening headache, stiff neck, nausea and vomiting, and low-grade fever for several days in the early October. There was no history of trauma, chills, night sweating or upper respiratory tract infection. Physical and neurological examinations as well as routine laboratory tests and chest radiograph were within normal limits. Blood culture for microorganisms was negative.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 6-years-old African American girl presented with severe headache for several days associated with vomiting, neck stiffness, fever, and unsteady gait. Physical examination was otherwise unremarkable. She was recently treated for otitis media approximately one week prior to admission. Mother reported that the patient had frequent headaches and incontinent of bowel and bladder during the past year. A lumbar puncture showed high CSF protein but no signs of infection. Computer Tomography (CT) (Figure 1) and Magnetic Resonance Imaging (MRI) of the brain (Figure 2) showed obstructive hydrocephalus with a 2.3 cm non-enhancing pineal region mass attached to the tectum. MRI of the spinal cord at this time was negative for metastatic disease (Figure 3).
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 6 year old girl from Medellin, Colombia, South America, presented with twenty-five days of left-sided headache, vomiting, and episodes of syncope lasting roughly five seconds. The patient had no other medical history of significance. She had no café au lait spots, and no other tumors or masses in other body sites. Neurological examination revealed no focal deficits. An MRI scan showed a large intra-axial left parietal lobe mass with significant surrounding edema. The mass did not appear to originate from the dura; it did reach or breach the pia on the parietal convexity, and medially close to the falx. The falx was pushed by the mass effect of the tumor and was clearly separate from it. (Fig 1). A surgical excision was done in Colombia, and a tentative diagnosis made. The slides and selected blocks were sent to the University of Missouri for consultation. Since the time of surgery, the patient has been treated with radiation (thirty treatments) and has done extremely well. Neurologically she is almost completely normal, and her mother reports that the patient is asymptomatic and leading a normal life attending school.
No restrictions on your remixing, redistributing, or making derivative works. Give credit to the author, as required.
Your remixing, redistributing, or making derivatives works comes with some restrictions, including how it is shared.
Your redistributing comes with some restrictions. Do not remix or make derivative works.
Most restrictive license type. Prohibits most uses, sharing, and any changes.
Copyrighted materials, available under Fair Use and the TEACH Act for US-based educators, or other custom arrangements. Go to the resource provider to see their individual restrictions.